
Yes. Hypertrophic cardiomyopathy is a leading cause of sudden cardiac death in young athletes and children, making it one of the most serious cardiac diagnoses a family can receive. But dangerous doesn’t mean hopeless. Most children with a confirmed HCM diagnosis can lead normal lives with proper treatment, careful monitoring and a management plan built around their specific risk profile by a paediatric cardiologist who actually understands the condition.
“HCM is one of those diagnoses that families come to me genuinely not knowing what to do with because the child looks well, plays normally and then you show them the echo and they can’t reconcile the two pictures at all,” says Dr. Prashant Bobhate, Pediatric Cardiologist in Mumbai, India.
What Makes HCM Dangerous in Children?
HCM thickens the heart muscle in ways that obstruct blood flow, destabilise the electrical system and in high-risk children create conditions for sudden cardiac death during activity nobody saw coming.
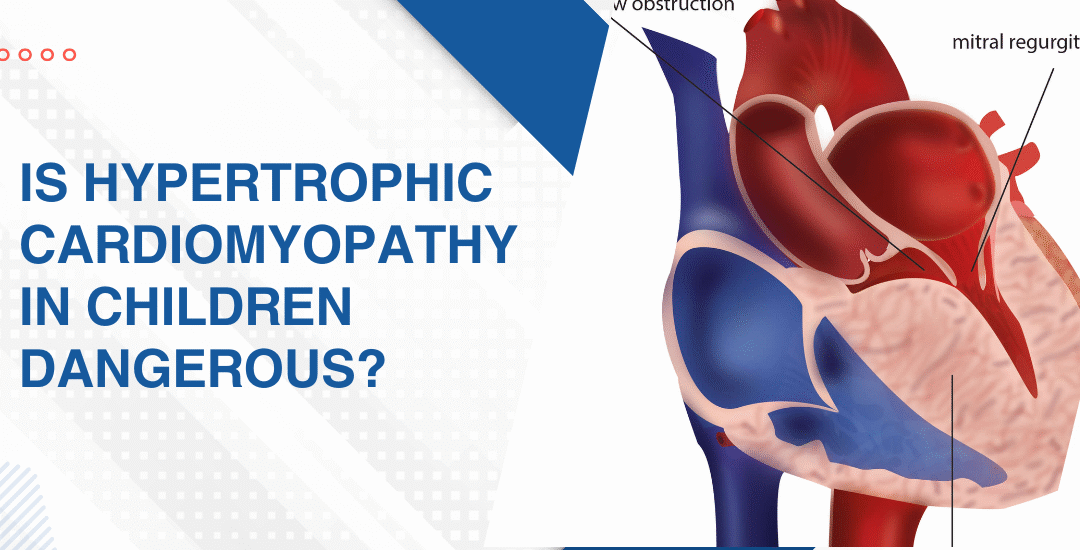
- Outflow obstruction: The thickened septum partially blocks blood leaving the heart and that blockage worsens under exertion when the heart needs more output not less.
- Dangerous arrhythmias: Disorganised muscle fibres create an unstable electrical substrate that can trigger ventricular fibrillation especially during physical stress in children with undiagnosed HCM.
- Diastolic dysfunction: The stiff thickened ventricle doesn’t relax properly between beats so filling is impaired even when the pumping function looks normal on a basic assessment.
- Mitral valve involvement: The abnormal septal bulge pulls the mitral leaflet into the outflow tract creating dynamic obstruction and mitral regurgitation simultaneously which significantly worsens the haemodynamic burden.
Every child with confirmed or suspected HCM needs a detailed structural assessment and 2D echocardiography for children maps the hypertrophy, outflow gradient and electrical risk before any management decision gets made.
How Is HCM Diagnosed and Managed in Children?
Diagnosis starts with an echo. Management depends entirely on severity.
- Genetic testing: First-degree relatives of any diagnosed child have a 50% chance of carrying the same mutation so family screening with ECG and echo is standard care not optional.
- Activity restrictions: High-intensity competitive sport in a child with significant outflow obstruction or arrhythmia risk is genuinely dangerous and restrictions must come from a specialist assessment not a general opinion.
- Medications: Beta-blockers and calcium channel blockers reduce the outflow gradient and improve diastolic filling making a real difference to exercise tolerance when titrated properly.
- ICD implantation: Children with prior cardiac arrest, sustained ventricular tachycardia or extreme hypertrophy on echo need an implantable defibrillator because medication alone doesn’t reliably prevent sudden death in high-risk cases.
Parents wanting to understand how early cardiac detection shapes HCM management should read this piece on whether a fetal echo can detect baby heart defects because identifying abnormalities early is always what expands the options available.
Why Choose Dr. Prashant Bobhate for HCM Care in Mumbai?
HCM in a child needs someone who can measure the outflow gradient under provocation, interpret Holter findings in the full clinical context and have the honest conversation about what sport means for that specific child’s risk profile. Not a generic restriction. A real assessment built around that one child. Dr. Prashant Bobhate has spent over 12 years managing complex paediatric cardiac conditions including hypertrophic cardiomyopathy, arrhythmia risk stratification and sudden cardiac death prevention across every age group at the Children’s Heart Centre, Kokilaben Dhirubhai Ambani Hospital.
Schedule a consultation to find out if a cure is possible and what the right treatment plan looks like for you.
FAQs
Can a child with HCM live a normal life?
Many can with proper monitoring and medication but the answer depends entirely on the degree of hypertrophy and individual arrhythmia risk assessed by a specialist.
Is HCM hereditary in children?
Yes, it follows an autosomal dominant pattern meaning every first-degree relative of a diagnosed child needs ECG and echo screening regardless of whether they have symptoms.
Can HCM cause sudden death in children during sports?
Yes and it’s one of the leading causes of sudden cardiac death in young athletes which is why every child with HCM needs a formal sport eligibility assessment before returning to competitive activity.
Does HCM get worse as a child grows?
It can because hypertrophy sometimes progresses during rapid adolescent growth which is why regular echo surveillance every one to two years is essential even in clinically stable children.
Can HCM cause sudden death in children during sports?
Yes and it’s one of the leading causes of sudden cardiac death in young athletes which is why every child with HCM needs a formal sport eligibility assessment before returning to competitive activity.
Does HCM get worse as a child grows?
It can because hypertrophy sometimes progresses during rapid adolescent growth which is why regular echo surveillance every one to two years is essential even in clinically stable children.
References:
- Hypertrophic Cardiomyopathy, MedlinePlus, U.S. National Library of Medicine — https://medlineplus.gov/hypertrophiccardiomyopathy.html
- Cardiomyopathy, National Heart Lung and Blood Institute — https://www.nhlbi.nih.gov/health/cardiomyopathy