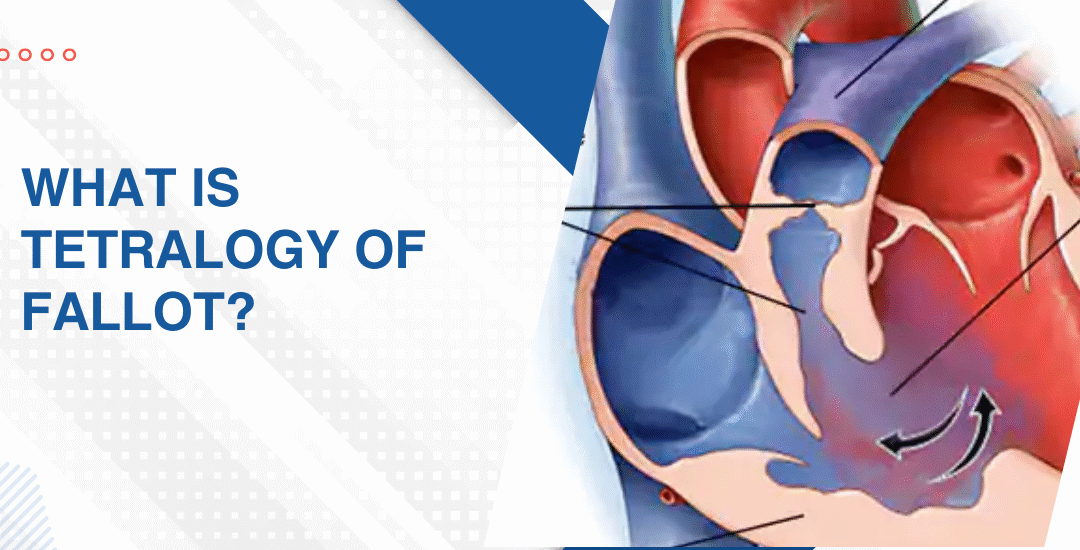
Early Symptoms of TOF in Babies
The earliest sign of Tetralogy of Fallot in babies is a bluish tint around the lips and fingertips caused by low oxygen in the blood. Babies with TOF also feed poorly, tire quickly, breathe faster than normal and don’t gain weight the way they should. Some are diagnosed before birth. Others make themselves known in those first weeks at home before anyone’s connected the dots.
“The blue around the lips is the sign most parents remember but TOF often announces itself more quietly first through a baby who just seems to be working too hard at everything,” says Dr. Prashant Bobhate, Pediatric Cardiologist in Mumbai, India.
What Are the First Signs of TOF That Show Up in a Baby?
Most parents don’t know what TOF looks like in those first days at home. And the earliest signs don’t walk in wearing a label. They show up in feeds, in breathing, in how hard that small body works doing things that should come easily.
- Blue colour: A bluish tint around the mouth or fingernails during feeding, crying or any effort is the signature sign and the one that tends to get a baby seen the same day.
- Fast breathing: A resting respiratory rate that consistently sits too high even when the baby is calm and undisturbed means the heart and lungs are working harder than they should be.
- Poor feeding: A baby who tires mid-feed, sweats during it or takes far too long to finish a small amount is burning energy the heart simply can’t replace fast enough.
- Tet spells: Sudden episodes where the baby turns deeply blue, becomes distressed or goes floppy during crying or feeding are TOF’s most urgent early sign and they don’t announce themselves in advance.
Catching these early is exactly what changes how the Tetralogy of Fallot conversation starts and how much time the surgical team has to work with before the situation becomes urgent.
What Other Early Signs Do Families Miss in TOF Babies?
The blue spells get all the attention. But the quieter signs that show up weeks before any tet spell are the ones families look back on and wish someone had connected earlier. They don’t look cardiac.
- Poor weight gain: A baby consistently falling off the growth chart despite adequate feeding and no obvious gut reason is often showing what chronic cardiac strain looks like from the outside.
- Visible effort breathing: Skin pulling in between the ribs with every breath means the work of breathing has gone up and the body is recruiting extra muscles just to keep oxygen coming in.
- Squatting behaviour: Once mobile a child with unrepaired TOF who instinctively squats during activity is doing something physiologically clever that temporarily pushes more blood toward the lungs without knowing why.
- Constant irritability: A baby who seems unsettled without obvious cause especially after feeds is often in a state of mild chronic oxygen deficit that makes everything feel uncomfortable in a way they can’t tell you about.
Parents seeing any of this at home should read this piece on how to spot the early signs of heart disease in neonates which goes through exactly what to watch for when everything still feels new and impossible to interpret properly.
Why Choose Dr. Prashant Bobhate for TOF Care in Mumbai?
Spotting TOF early is only part of it. What comes next depends entirely on who’s reading the echo, planning the repair and managing everything between diagnosis and the operating table. Dr. Prashant Bobhate spent over 12 years working with children at every stage of congenital heart disease. TOF from fetal diagnosis through surgical planning through long term follow up. Trained at Escorts Heart Institute in New Delhi then went deliberately to the University of Alberta in Canada for advanced paediatric cardiac fellowship training. His team performed India’s very first successful Transcatheter Potts Shunt and actively manages over 400 children on advanced cardiac therapy right now. He doesn’t just diagnose and hand you a referral letter. He stays in the room for everything that comes after.
Schedule a consultation to find out if a cure is possible and what the right treatment plan looks like for you.
FAQs
When do TOF symptoms appear?
Most babies show symptoms within the first few weeks to months of life though some are diagnosed before birth through fetal echocardiography.
Is lip blueness always TOF?
Not always but cyanosis in any baby always needs urgent cardiac evaluation that day regardless of the suspected cause.
Can TOF be missed at birth?
Yes. Mild TOF can pass routine newborn screening which is why persistent poor feeding, fast breathing or blueness during effort needs cardiac follow up without delay.
Is TOF fatal without surgery?
Without repair risks increase significantly over time but children who get complete surgical repair between 3 and 6 months go on to live normal active lives.
References:
- Tetralogy of Fallot, MedlinePlus, U.S. National Library of Medicine — https://medlineplus.gov/ency/article/001567.htm
- Congenital Heart Defects in Children, National Heart Lung and Blood Institute — https://www.nhlbi.nih.gov/health/congenital-heart-defects