
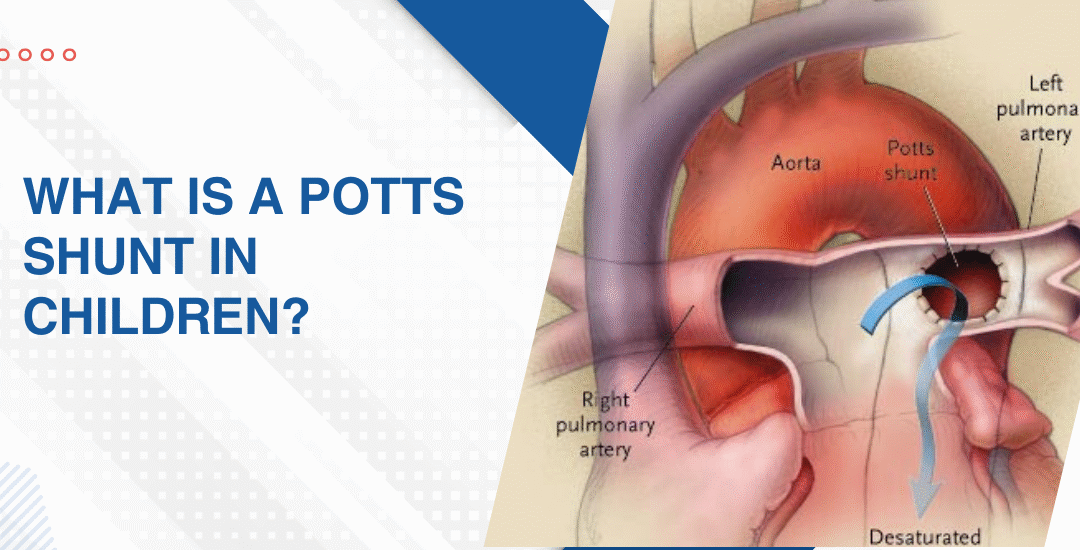
The Potts shunt is a surgically or catheter-created connection between the left pulmonary artery and the descending aorta that gives the right ventricle a pressure release valve when pulmonary hypertension has become so severe the right heart can no longer sustain it safely on its own. It doesn’t cure pulmonary hypertension.
“The Potts shunt is one of the most misunderstood procedures in paediatric pulmonary hypertension care because families hear it described as a last resort and immediately interpret that as giving up when it’s actually the opposite.” says Dr. Prashant Bobhate, Pediatric Cardiologist in Mumbai, India.
What Does the Potts Shunt Actually Do for a Child's Heart?
It creates a deliberate right-to-left shunt at the level of the great vessels that allows the overloaded right ventricle to decompress directly into the aorta rather than continuing to push against a pulmonary vascular resistance it can no longer overcome.
- Right ventricular decompression: The shunt allows blood to bypass the high-resistance pulmonary circulation entirely which immediately reduces the pressure load on a right ventricle that was heading toward failure and gives the chamber a chance to recover function it was rapidly losing.
- Maintains cardiac output: A failing right ventricle in severe PH can no longer maintain adequate systemic circulation and the Potts shunt preserves overall cardiac output even at the cost of some arterial oxygen desaturation which is an acceptable trade-off when the alternative is right heart collapse.
- Bridge to transplant: In children who are maxed out on medical therapy and deteriorating despite everything, the Potts shunt buys enough haemodynamic stability to reach lung transplant listing criteria and survive the wait in a condition where transplant is actually still feasible.
- Transcatheter approach: India’s first successful transcatheter Potts shunt was performed at this centre using a catheter-based technique rather than open surgery which reduces the procedural risk significantly in children who are already haemodynamically fragile and couldn’t safely tolerate a sternotomy at that point in their disease.
Understanding what interventional options exist for children with severe pulmonary hypertension who have exhausted conventional medical pathways is exactly what a thorough interventional treatment for pulmonary hypertension assessment maps out before any decision gets made.
Which Children With PH Actually Need a Potts Shunt?
A very specific group. Not every child with PH. Not even every child with severe PH.
- Suprasystemic RV pressure: Children whose right ventricular pressure has risen above systemic pressure on maximal combination medical therapy are the primary candidates because at that level the right heart is in imminent danger of irreversible failure and the shunt is the only intervention that immediately addresses the mechanical crisis.
- Failing on maximal therapy: A child already on triple combination PH therapy including a prostacyclin who continues to deteriorate clinically and haemodynamically is telling you the medical ceiling has been reached and the next decision is either the Potts shunt or palliative management with no bridge to anything.
- Pre-transplant stabilisation: Children being evaluated for lung transplant who are too unstable to survive the wait on medical therapy alone are given the Potts shunt to stabilise their haemodynamics long enough to get listed, wait and reach the transplant in a condition where it can actually succeed.
- Not suitable for everyone: Children with significant left heart disease, severe aortic regurgitation or unfavourable anatomy at the shunt site aren’t candidates and the decision requires detailed catheterisation data, imaging and a team that has actually performed this procedure rather than read about it.
Parents wanting to understand how severe pulmonary hypertension can progress and why options like Potts shunt may become necessary should also read about when lung transplant is needed in pulmonary hypertension.
Why Choose Dr. Prashant Bobhate for Potts Shunt and Severe PH Care in Mumbai?
Dr. Prashant Bobhate performed India’s first successful transcatheter Potts shunt and has over 12 years of expertise managing complex paediatric pulmonary hypertension cases at Kokilaben Dhirubhai Ambani Hospital, including advanced interventions, triple therapy management, transplant bridging, and severe cases requiring specialised multidisciplinary pulmonary hypertension care.
Schedule a consultation to find out if a cure is possible and what the right treatment plan looks like for you.
FAQs
Is the Potts shunt a cure for pulmonary hypertension in children?
No, it’s a pressure relief procedure that reduces right ventricular strain and buys time but the underlying pulmonary vascular disease continues and medical therapy must be maintained alongside it.
How is a transcatheter Potts shunt different from surgical Potts shunt?
The transcatheter approach creates the same shunt through a catheter without opening the chest which significantly reduces procedural risk in children who are already haemodynamically compromised and couldn’t safely tolerate open surgery.
Which hospital in Mumbai performs the Potts shunt for children?
The Children’s Heart Centre at Kokilaben Dhirubhai Ambani Hospital where India’s first transcatheter Potts shunt was performed is one of the very few centres in the country with experience in this specific procedure.
Can a child live normally after a Potts shunt?
Most children have improved exercise tolerance and quality of life after the shunt due to right ventricular decompression but they remain on PH medications and require close ongoing specialist follow up indefinitely.
References:
- Pulmonary Arterial Hypertension, National Heart Lung and Blood Institute — https://www.nhlbi.nih.gov/health/pulmonary-hypertension
- Pulmonary Hypertension, MedlinePlus, U.S. National Library of Medicine — https://medlineplus.gov/pulmonaryhypertension.html