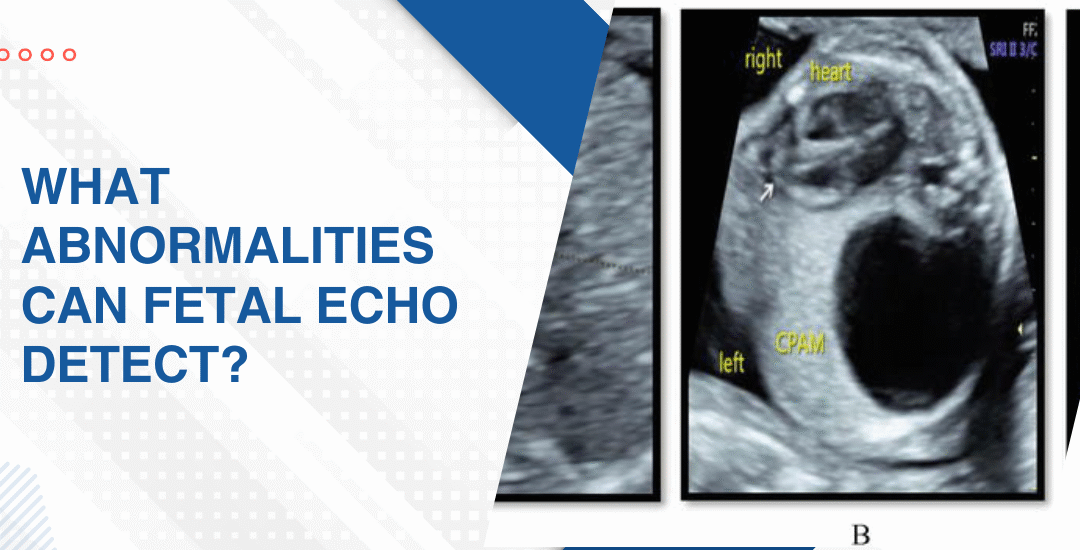
Is Fetal Echocardiogram Safe for the Baby
Yes. A fetal echocardiogram is completely safe for both the baby and the mother. It uses standard ultrasound technology with no radiation involved and no known risk at any stage of pregnancy. The same technology that’s been used in routine pregnancy scans for decades. Just applied more carefully and for longer to look specifically at the heart.
“A fetal echo uses the exact same ultrasound waves as a routine pregnancy scan. There is no radiation. No risk to the baby. Just a longer, more detailed look at a heart that deserves that attention,” says Dr. Prashant Bobhate, Pediatric Cardiologist in Mumbai, India.
Why Is a Fetal Echo Safe and What Does It Actually Involve?
Most parents asking this question aren’t really asking about physics. They’re asking whether something is going to hurt their baby. And the honest answer is no. Nothing about this scan puts your baby at risk in any way.
- No radiation whatsoever: Unlike X-rays or CT scans a fetal echocardiogram uses only sound waves to build its images and sound waves don’t damage tissue, don’t affect developing cells and don’t accumulate in the body in a way that causes any problem at all.
- Same technology as a routine scan: The transducer pressed against the abdomen is identical to what gets used in every standard pregnancy ultrasound and the only difference is the operator’s focus, the duration and how carefully those heart structures get examined frame by frame.
- Can be repeated without concern: If the baby’s position makes imaging difficult the first time or if a follow up scan is needed to monitor a finding there’s no limit on how many times a fetal echo can be safely done and no cumulative risk that builds up with repeat scans.
- No needles, no sedation, nothing invasive: The entire scan happens externally through the mother’s abdomen and in some cases a transvaginal probe is used for earlier scans but nothing enters the uterus, nothing touches the baby and nothing about the process is invasive at any point.
Understanding what the scan actually involves is what makes fetal echocardiography feel like something you’re walking into with your eyes open rather than something that was just added to your appointment list without any real explanation.
What Should You Actually Expect During and After a Fetal Echo?
Because the safety question is usually followed by a practical one. What actually happens in that room. How long is it. Will something feel wrong. And what do you do if the scan finds something you weren’t expecting to hear about that day.
- The scan takes 30 to 60 minutes: Longer than a routine anomaly scan because the cardiologist is examining every chamber, every valve, every vessel and watching blood flow in real time rather than taking a quick look and moving on to the next item on the checklist.
- You’ll feel nothing unusual: Warm gel on the abdomen, a transducer pressed gently against the skin and a lot of quiet concentration from the person doing the scan. Some babies cooperate immediately. Others take their time settling into a position that shows what needs to be seen.
- Results are usually discussed the same day: A paediatric cardiologist performing the scan can give you a clear picture of what was found or what wasn’t found before you leave the room and that conversation is often the part families feel most unprepared for regardless of what the answer turns out to be.
- A normal result is genuinely reassuring: Not a perfect guarantee because some very small defects only become visible after birth but a normal fetal echo from an experienced specialist means the vast majority of significant structural problems have been looked for and not found.
Parents in a high risk category wanting to understand what happens if something does get found during the scan should read this piece on importance of fetal diagnosis of critical congenital heart disease which explains honestly what an early prenatal finding actually changes about the care plan and the options available to families from that point.
Why Choose Dr. Prashant Bobhate for Fetal Echocardiography in Mumbai?
A fetal echo being safe doesn’t mean every fetal echo is equally useful. The safety is in the technology. The value is entirely in the person reading it. Dr. Prashant Bobhate trained at Escorts Heart Institute in New Delhi then went specifically to the University of Alberta in Canada for advanced paediatric cardiac fellowship training. Over 12 years reading these scans and then following those same babies through every stage of what came after. His team performed India’s very first successful Transcatheter Potts Shunt and actively manages over 400 children on advanced therapy right now. He doesn’t just tell you the scan was normal or abnormal. He tells you what it actually means for your specific baby and what needs to happen next because of it.
Schedule a consultation to find out if a cure is possible and what the right treatment plan looks like for you.
FAQs
Does fetal echo use radiation?
No. It uses only sound waves exactly like a routine pregnancy ultrasound and there is no radiation involved at any point which means there is no radiation related risk to the baby or mother whatsoever.
Can fetal echo be done multiple times in one pregnancy?
Yes without any concern. There is no cumulative risk from repeat fetal echocardiograms and if follow up scans are needed to monitor a finding they can be scheduled as many times as clinically necessary.
Does the baby feel anything during the scan?
No. The scan is entirely external through the mother’s abdomen and uses sound waves that the baby cannot feel in any way that differs from the ordinary sound environment of the womb.
What if my baby moves too much during the scan?
The sonographer waits for a better position and the scan continues when the baby settles because image quality matters more than speed and no part of the scan can be rushed without compromising what can actually be seen.
References:
- Fetal Echocardiography Overview, MedlinePlus, U.S. National Library of Medicine — https://medlineplus.gov/ency/article/003813.htm
- Congenital Heart Defects, National Heart Lung and Blood Institute — https://www.nhlbi.nih.gov/health/congenital-heart-defects