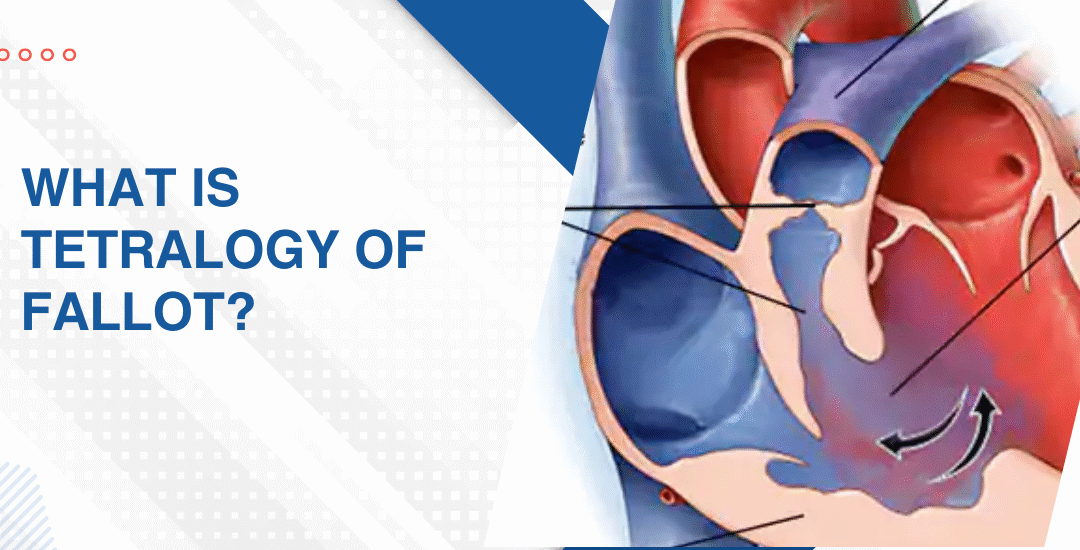
What Is Tetralogy of Fallot?
Tetralogy of Fallot is a congenital heart condition made up of four specific structural defects that occur together inside the heart from birth. It reduces the oxygen reaching the blood and it’s one of the most common serious heart defects found in children. Scary name. But genuinely one of the most treatable cardiac diagnoses a child can receive.
“Tetralogy of Fallot sounds overwhelming the first time you hear it but these four defects are well understood and children who get the right surgical repair at the right time do genuinely well,” says Dr. Prashant Bobhate, Pediatric Cardiologist in Mumbai, India.
What Are the Four Defects That Make Up Tetralogy of Fallot?
The name literally means four. And understanding what each of those four things does to blood flow inside your child’s heart is what makes everything a specialist says from that point forward actually land properly.
- Ventricular septal defect: A hole between the two lower chambers lets oxygen-poor blood mix with oxygen-rich blood before it even leaves the heart and that mixing is exactly what drives the low oxygen levels that show up on the skin and lips as that bluish colour most families notice first and can’t unsee after.
- Pulmonary stenosis: The valve leading from the heart toward the lungs is narrowed and sometimes the entire passage below it is narrowed too which means the right side of the heart is pushing far harder than it was ever built to just to get blood through to the lungs at all.
- Right ventricular hypertrophy: Because the right side works so much harder against that narrowed outflow the muscle wall thickens trying to keep up. It’s the heart doing its absolute best to compensate for a situation it genuinely cannot fix on its own no matter how hard it tries.
- Overriding aorta: The aorta sits shifted directly over the hole between the chambers instead of sitting entirely over the left side where it belongs and this means it pulls blood from both chambers simultaneously rather than only the clean oxygenated blood it was designed to carry.
These four things together are what makes Tetralogy of Fallot a condition that needs surgical correction rather than watchful waiting and the earlier that correction happens the better and faster the heart bounces back from it.
What Are the Signs of Tetralogy of Fallot and How Is It Treated?
Some children with TOF are diagnosed before birth. Others come to attention in those first fragile weeks at home. And occasionally a milder form gets missed entirely until a child is older and something just keeps not adding up no matter how many times it gets explained away.
- The blue spells nobody forgets: Tet spells are sudden episodes where the baby turns deeply blue, becomes distressed or goes floppy and they happen when the narrowed pulmonary outflow drops blood oxygen dramatically in a way that doesn’t wait for a convenient moment to do it.
- Squatting in older children: A child with unrepaired TOF who instinctively squats during activity is doing something physiologically clever without knowing it because squatting increases lower body resistance and briefly pushes more blood toward the lungs to boost oxygen when the body needs it most.
- Surgical repair usually between 3 and 6 months: Most centres repair TOF in the first six months of life with a complete repair that closes the VSD, widens the pulmonary outflow and repositions the aorta all in one operation rather than staging it across multiple procedures over years.
- Outcomes after repair are excellent: Children who get complete TOF repair at the right time grow up to live normal active lives and while lifelong cardiac follow up is part of the picture the vast majority reach adulthood with genuinely good heart function and no meaningful limitations on how they live.
Parents wanting to understand what early cardiac warning signs actually look like before any diagnosis gets made should read this piece on how to spot the early signs of heart disease in neonates which goes through what these signs genuinely look like in those first weeks at home when everything still feels new and impossible to interpret properly.
Why Choose Dr. Prashant Bobhate for Tetralogy of Fallot Care in Mumbai?
A TOF diagnosis needs someone who has spent years specifically inside complex congenital cardiac disease. Not someone applying a general protocol to a condition that has never once responded well to general anything. Dr. Prashant Bobhate trained at Escorts Heart Institute in New Delhi then went deliberately to the University of Alberta in Canada for advanced paediatric cardiac fellowship training. Over 12 years working with children at every stage and complexity of congenital heart disease. His team performed India’s very first successful Transcatheter Potts Shunt and actively manages over 400 children on advanced therapy right now. He doesn’t give families a standard answer pulled from a protocol sheet. He looks at your child’s specific anatomy and builds the plan entirely from what he actually finds there.
Schedule a consultation to find out if a cure is possible and what the right treatment plan looks like for you.
FAQs
Can TOF be detected before birth?
Yes. Fetal echocardiography between 18 and 24 weeks can identify TOF before birth which allows families to plan delivery at a specialist centre with a paediatric cardiac team ready from the very first moment rather than scrambling after the fact.
Is surgery always needed for TOF?
Yes always. TOF can’t be managed with medication alone and complete surgical repair closing the VSD and widening the pulmonary outflow is the only thing that actually resolves the four underlying structural problems properly.
Can a child with repaired TOF play sports?
Most can participate in normal physical activity and the specific level of exercise allowed is determined through regular cardiac follow up rather than a blanket restriction applied to every child the same way regardless of their individual situation.
What's the long term outlook after TOF repair?
Excellent for the vast majority. Most children who get complete repair in infancy grow into adults with good heart function though lifelong follow up is needed to monitor the pulmonary valve and right heart as they get older.
References:
- Tetralogy of Fallot, MedlinePlus, U.S. National Library of Medicine — https://medlineplus.gov/ency/article/001567.htm
- Congenital Heart Defects in Children, National Heart Lung and Blood Institute — https://www.nhlbi.nih.gov/health/congenital-heart-defects